75 year old male with altered sensorium
75 yr old male patient came to the casuality at 9:30 am on 7/11/21 with c/o altered sensorium since yesterday night.
Patient has 3 sons, is a farmer by occupation, stopped going to work since 3 years due to old age.
He was able to perform all his daily activities on his own.
Pt was apparently asymptomatic till yesterday evening, had dinner and went to sleep. Around 12 am pt suddenly made noises ( like snoring ) and had involuntary movements for 2 mins. From then the patient is unconscious and not responding ( sudden onset )
No h/o tongue bite, no involuntary micturition.
No previous history of seizures.
No previous history of fever and patient was active till yesterday.
Immediately pt was taken to hospital in Nalgonda and was referred here.
No H/o vomiting , headache
K/c/o DM since 10 years (on medication)
Not a k/c/o HTN, CAD, CVA, Asthma
Personal history:
Diet- mixed
Sleep- adequate
Appetite- normal
Bowel and bladder movements- regular
Addictions-
H/o cigarette smoking for 15 years. Stopped 3 years ago
H/o occasional alcohol intake. Stopped 3 years ago.
Vitals:
Temperature- 102.9 F
BP- 140/80 mmhg
PR- 111 beats / min
RR- 20 cpm
Spo2- 92 % @ 14 L O2
GRBS- 329 mg/dl
O/E
No signs of pallor, icterus, cyanosis clubbing, edema, lymphadenopathy.
No malnutrition/dehydration
CVS - S1 S2 +. No murmurs
RS- BAE+
Barrel shaped chest +
B/L crepts + in all lung fields
P/A- scaphoid, soft, non tender
No organomegaly


CNS-
Level of consciousness- coma
GCS E1V1M1
Pupils mid dilated. Not reacting to light
Gag+
neck stiffness +
Reflexes. Rt. Lt
Biceps. 2+. 2+
Triceps. 2+. 2+
Supinator. 1+. 1+
Knee. 2+. 2+
Ankle. 1+. 1+
Plantar. Withdrawing mute
Provisional diagnosis:
Altered sensorium under evaluation
Sepsis secondary to ? Aspiration pneumonitis
? Old CVA
COPD
K/c/o Diabetes Mellitus since 10 years
Investigations:
Hb-13.8
TLC-10,800
PLC-3,00,000
PT- 17
INR- 1.2
APTT- 33
Blood group - A +
UKB- negative
Alb- 2+
Sug- trace
PC- 4-6
EC- 2-4
ABG-
PH- 7.314
PCO2-27.9
PO2-47.1
HCO3- 13.8
Urea-55
Creat- 1.8
Uric acid- 7.0
Ca- 9.5
Po4- 4.0
Na- 141
K- 3.7
Cl- 102
RBS- 332 mg/dl
HbA1c- 7.2%
HIV, HbsAg, HCV- negative
RAT for covid 19- negative
ECG

CT BRAIN:
Hypodensity of bilateral cerebellar hemispheres and brain stem

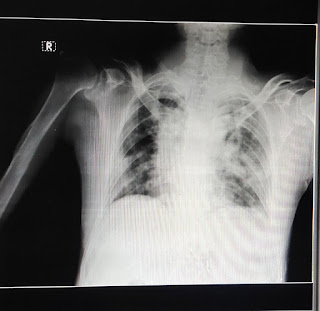
X ray chest:
B/L consolidation of lungs ( lt > rt )
Treatment
IVF- NS, RL @ 75 ml/ hr
Inj piptaz 4.5 g IV STAT Followed by 2.25 g IV QID
Inj Neomol 1 g IV SOS if temp > 101F
Inj PAN 40 mg IV/ OD
Inj Zofer 4 mg IV/TID
Inj Optinueron 1 amp in 100 ml NS IV/OD
RT- feeds 2nd hourly
3 scoops protein powder+ 150 ml milk
Oral suctioning -3rd hourly
Inj Midaz 0.02 - 0.1 mg/kg/hr
Pt was intubated I/v/o low GCS and falling Spo2.
ACMV mode:
Fio2- 100
PEEP- 6
vT- 450
RR- 14
Post intubation :
GCS- E1 VT M1
Dolls eye- negative
ABG-
PH- 7.235
PCO2-41.3
PO2-292
HCO3- 16.7
Post intubation X-ray

Patient is comatosed ,also under sedation with midaz .
On mechanical ventilation - ACMV - VC mode -
RR-14/ min
Fio2-80%
VT-400 ml
PEEP -7
O-Afebrile
GCS -E1VTM1
Right eye -mature cataract
Left eye pupils - reacting to light +
PR-96/min
RR-21/ min
BP-110/80 mmHg
GRBS -222 mg/dl
RS - BAE + , bilateral infraxillary fine crepts +
Barrel shaped chest
CVS - S1,S2 heard
CNS - comatosed
No response to deep painful stimuli.
Dolls eye absent
Gag reflex +
Reflex - Rt. Lft
B- 2+. 2+
T-. 2+. 2+
S. +1. +1
K +2. +2
A. +1. +1
Pl. W. Mute
Mrng ABG - severe metabolic acidosis -
PH -7.1 with HcO3-10.3
HIGH ANION GAP -28
LP was done yesterday -
With counts -10 cells , Lymphocytes ,
Sugars -198
Protein -90 - increased
? Viral meningitis

A- Altered sensorium under evalation -? Viral meningitis
High Anion gap metabolic acidosis
Renal failure - ? AKI
Known Diabetic since 10 years
Treatment -
1- Iv fluids
2- Nebulisation with duolin and Budecort
3- GRBs monitoring and insulin according to sugars
4- Inj .Piptaz 2.25gm / IV / QID
Day 3:
Patient is comatosed ,
On mechanical ventilation - ACMV - VC mode -
RR-25/ min
Fio2-80%
VT-400 ml
PEEP -7
O-febrile- temp-104 F
Fever spikes +
GCS -E1VTM1
Right eye -mature cataract
Left eye pupils - reacting to light +
PR-124 /min
RR-24/ min
BP-170/90 mmHg
I/O- 5400/2350 ml
GRBS -254 mg/dl
RS - BAE + , bilateral infraxillary fine crepts +
Barrel shaped chest
CVS - S1,S2 heard
CNS - comatosed
No response to deep painful stimuli.
Dolls eye absent
Gag reflex +
Reflex - Rt. Lft
B- 2+. 2+
T-. 2+. 2+
S. +1. +1
K +2. +2
A. +1. +1
Pl. W. Mute
Mrng ABG - compensated metabolic acidosis
A- Altered sensorium under evalation -Secondary to PCA stroke( cerebellum and brain stem )
CKD
- sepsis -? Aspiration pneumonia
K/c/o diabetes since 10 years
Treatment -
1- Iv fluids
2- Nebulisation with duolin and Budecort
3- GRBs monitoring and insulin according to sugars
4- Inj .Monocef 2gm/IV/BD .
Day 4:
S:
Fever spikes+
O:
E1VTM1
Temp- 101.1F
BP-160/100 mmhg
PR- 117 bpm, regular
CVS- S1 S2+ no murmurs
RS- NVBS + decreased breath sounds B/l ISA
I/O- 3900/2100 ml
RR- 21 cpm
Spo2- 98% with fio2 50%
SIMV MODE:
fio2- 50%
PEEP- 5 cm H2O
VT- 420 ml
CNS
Reflexes. Rt. Lt
Biceps. 1+. 1+
Triceps. - -
Supinator. - -
Knee. - -
Ankle. - -
Plantar. Mute mute
Corneal and conjunctival reflexes absent
Dolls eye- absent
Gag- absent
Hb-12.1
TLC-13600
Plc-1.40
Urea -64
Creat-1.6
Na- 147
K-3.7
Cl- 103
CA- 8.3
P- 2
TB-1.12
DB-0.18
AST-122
ALT-59
TP-4.9
Alb- 2.8
A/G-1.39
A:
Hypodensity in b/l cerebellar and brainstorm
? Viral meningitis
? AKI secondary to sepsis ? Aspiration pneumonia
? Consolidation
With grade I bed sore
P:
IVF
Nebulisation with duolin and budecort
Inj Neomol IV if temp> 101F
Inj Optineuron
Inj pantop 40 mg IV/OD
inj Ceftrioxone 2 gm IV/OD
Inj HAI 40 IU in 39 ml NS
Tab Amlong 5 mg RT OD
RT feeds 2nd hourly


Comments
Post a Comment